Running with Crohn’s: Fistula
Typical warnings apply.
This entry includes graphic descriptions of the nether end of the human
digestive tract, the functions of that tract, and the surgical
interventions required to treat fistulas.
A fistula is an abnormal connection between body cavities or
organs of the body. Fistulas can connect
things like your intestines to your bladder, vagina, uterus, skin, or any other
organ. Because these connections are abnormal,
they usually cause severe medical problems.
The fistula itself is an open wound. Since my fistula connects to the colon, fecal
matter passes through the fistula. As
you can imagine, putting crap in an open wound leads to infections. It also means that fecal matter passes all the way
through the fistula and leaks out. I deal with this leakage using feminine pads. While this seemed very *odd* and unmanly (?) the first time I used pads for this purpose, it seems a very natural and *practical* method of dealing with the problem now. My wife and I actually joke about it now. For men worried about this showing, I have had no issues with the pads showing through my shorts. However, I am a bit worried about the new body scanners in airports. The way I deal with these is I take the pad off and throw it away in the restroom right before the security check point, then I go through the check point, and then I pull a new pad out of my carry-on bag and put it on in the bathroom after the security check-point.
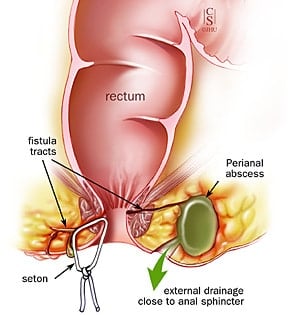
 Illustration of an anorectal fistula. Note the fistula begins as an infected pouch that gradually widens and grows in length until it reaches the outside. My fistula actually exits the muscle and then runs between the muscle and skin for 1-2 inches before opening.
Illustration of an anorectal fistula. Note the fistula begins as an infected pouch that gradually widens and grows in length until it reaches the outside. My fistula actually exits the muscle and then runs between the muscle and skin for 1-2 inches before opening.
I have had three fistulas and had my third surgical intervention
on my third fistula on July 31. All
three of my fistulas connect my colon with my skin. The fistula began in the colon and slowly
grew in length until it erupted within about two inches of my anus. My previous two fistulas burrowed through
skin without actually penetrating the rectal muscle walls. Unfortunately, my latest fistula burrowed all
of the way through both rectal muscle groups.
There are several different treatment options for fistula;
however, they are all surgical. However,
before attempting to correct the fistula, the doctor must first ensure the
fistula is as free of infection as possible.
Since this third fistula had abscessed, my first surgical intervention
involved simply cutting open the fistula and draining the abscess. My second surgical intervention included running
a specially designed probe up through the fistula both to map it out and to
place a rubber band like object (called a seton). The purpose of the seton is to hold the
fistula open so that as much of the infection as possible can drain out.

The possible approaches to fix fistulas include:
- Cauterize or suture closed the interior opening of the fistula, and then permit it to heal from the inside out
- If the fistula only runs under the skin, cut open the fistula pathway
- Inject Fibrin glue along the entire length of the fistula
- Insert a specially designed plug at the point the fistula penetrates the muscle wall
- Insert a specially designed plug at the point the fistula penetrates the muscle wall and surgically modify the muscle wall to accept the plug
- Surgically close the fistula and reconstruct the muscle wall

Fibrin glue

Fistula plug
As I understand it, the surgeon used the second approach for
my fistula – it was extremely painful. The
surgeon used the first approach for my second fistula (MUCH less painful). For my third fistula, after draining the
infection, the surgeon used the Fibrin glue injection (also relatively pain
free).
For my situation, the chances of the Fibrin glue injection
successfully closing the fistula are remote (~20%). The chances for a simple plug placement
working are only about 40%. Therefore,
it seems likely that I will require a more invasive surgical intervention.
Le sigh
My other posts on fistulas
Fistula post-op
Suture removal and fistula check-up
Fistula incision and drainage